

Arginase-1 (SP156)
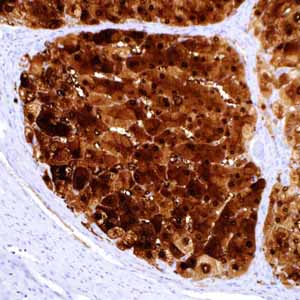
Hepatocellular carcinoma (HCC) is the most common primary malignant tumor of the liver accounting for an estimated 70%-85% of total liver cancers worldwide1,2. While the highest liver cancer rates are found in East and Southeast Asia and sub-Saharan Africa, the incidence is increasing in the West due to the burden of chronic hepatitis C infection and steatohepatitis attributed to the obesity epidemic1,3. Although advancements in diagnostic imaging modalities and refined methods of clinical investigation have obviated the need for tissue diagnosis in some cases4,5, fine needle aspiration (FNA) biopsy remains the procedure of choice in the assessment and diagnosis of focal liver nodules and masses2. Unfortunately, diagnostic pitfalls exist in the morphologic distinction of HCC from other hepatocellular and non-hepatocellular mass lesions. Of note, the morphologic distinction of regenerative cirrhotic nodules, hepatic adenoma, and focal nodular hyperplasia from well-differentiated HCC presents a diagnostic challenge, particularly in small biopsies with limited sampling. Similarly, cases of metastatic carcinoma and other benign and malignant non-hepatocellular mimics are well documented and can be problematic4-7. In difficult or equivocal cases, the application of immunohistochemical (IHC) panels has been shown to aid in the distinction of benign and malignant liver lesions4-9. In particular, the application of CD10, polyclonal carcinoembryonic antigen, alpha-fetoprotein, HepPar-1, and glypican-3 (GPC-3) IHC has proven valuable in liver biopsy and FNA cytology specimens5-10. IHC staining for HepPar-1, a mitochondrial urea cycle antigen, has demonstrated high sensitivity and specificity in the distinction between metastatic carcinoma and HCC but is also expressed in benign hepatocellular lesions8,9. In contrast, GPC-3, a heparin sulphate proteoglycan expressed at high levels in HCC, has shown high specificity with suboptimal sensitivity in the diagnosis of HCC when used in isolation. Arginase-1 is a key urea cycle metalloenzyme that has demonstrated expression in normal human liver with a high degree of specificity11,12. In sections of normal liver, anti-arginase-1 produced strong, diffuse cytoplasmic reactivity in all hepatocytes throughout the lobule. In a small percentage of cases, patchy nuclear reactivity is also evident in hepatocytes along with the strong cytoplasmic reactivity. There is no reactivity in bile duct epithelial cells, sinusoidal endothelial cells, Kupffer cells, or vascular endothelial cells. In sections of HCC, anti-arginase-1 produces either cytoplasmic or cytoplasmic plus nuclear reactivity.