

CD117, c-kit (YR145)
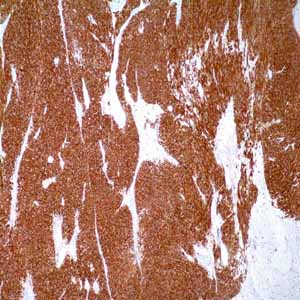
CD117, c-kit is a tyrosine kinase receptor found on interstitial cells of Cajal, germ cells, bone marrow cells, melanocytes, and mast cells. CD117 expression by immunohistochemistry is considered a key diagnostic feature in gastrointestinal stromal tumors (GISTs) and is seen in most of these tumors. The staining pattern of CD117 expression in GISTs is typically strong and diffuse, showing a pancytoplasmic and sometimes membranous pattern. In addition, some GISTs, especially extraintestinal or epithelioid GISTs show a cytoplasmic ‘‘dotlike’’ immunostaining pattern.1 When used in combination with other markers, the sensitivity and specificity of CD117 antibody increases. The panel, including CD117, CD34, S-100, desmin, and SMA, can effectively differentiate between GISTs, true smooth-muscle tumors, and neural tumors, because GISTs do not typically express desmin or S100, but demonstrate immunopositivity for CD117 and/or CD34 and occasionally SMA. Therefore, within the spectrum of mesenchymal neoplasms of the GI tract, CD117, CD34, desmin, S-100, and SMA should be the primary panel of the choice for most circumstances.2 A common, morphologically, and clinically important differential diagnosis of germ cell tumors is the distinction of seminoma from embryonal carcinoma. A 2-antibody panel, CD117 and CD30 with opposite patterns of reactivity, is recommended and CD117 can be demonstrated in 95% to 100% of seminoma as well as intratubular germ cell neoplasia, but is negative in almost all embryonal carcinoma.3 The morphologic distinction of clear cell renal cell carcinoma (RCC), chromophobe RCC, eosinophilic and oncocytoma sometimes generates difficulties, especially for high grade tumors. A panel of three antibodies, including CD117, CK7 and CA IX, would help to separate them. Clear cell RCC will display diffuse membranous staining of the tumor cells by CA IX, but is negative for CD117 and CK7; chromophobe RCC will be positive for CK7 (cytoplasmic) and CD117 (membranous); whereas CD117 highlights oncocytoma in the membrane, but is almost completely negative for CK7.4 Disorders of mast cells, although uncommon, can be difficult to diagnose because of morphologic overlap with other diseases such as B-cell and T-cell lymphomas, acute and chronic myelogenous leukemia, myelodysplastic syndromes, and histocytic proliferations. Mast cells are well known to show distinctive membranous and cytoplasmic staining for CD117. Furthermore, similar staining is seen in mast cell disorders and can be used to identify neoplasms of mast cells in bone marrow, skin, lymph nodes, and solid organs.5