

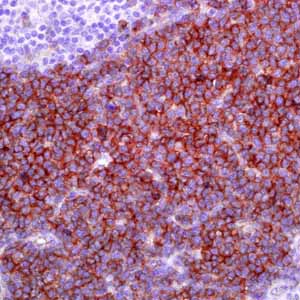
CD123 (6H6)
Blastic plasmacytoid dendritic cell neoplasm (BPDCN), previously known as CD4+/CD56+ hematodermic neoplasm or blastic NK-cell lymphoma, is a malignant neoplasm composed of immature hematopoietic precursors of plasmacytoid dendritic cells.1 The most frequent manifestation is a skin lesion, bone marrow involvement, and regional lymphadenopathy.1 Myeloid leukemia cutis (LC), myeloid sarcoma, and large aggressive B cell lymphomas should be differentiated from BPDCN. Recently, it has been reported that these entities can be distinguished by using immunohistochemistry (IHC) in paraffin-embedded tissue sections.2 In this study, 23 myeloid LC and 12 BPDCN cases were evaluated using a panel of antibodies against CD123, TCL1, CD4, CD56, MPO and CD33; with results as follows: anti-CD123 stained 4 cases (17%) of myeloid LC and 10 cases (83%) of BPDCN; anti-TCL-1 stained 2 cases (9%) of myeloid LC and 9 (82%) of 11 cases of BPDCN; anti-CD4 stained 2 cases (9%) of LC and all 12 cases (100%) of BPDCN; anti-CD56 stained 12 cases (52%) of LC and all 12 cases (100%) of BPDCN; anti-myeloperoxidase stained 7 cases (30%) of LC and 0 cases (0%) of BPDCN. Anti-CD33 was not helpful; it stained 18 (78%) cases of LC and 11 cases (92%) of BPDCN. The results indicated that a panel that includes antibodies against CD4, CD56, CD123, and TCL-1 can appropriately distinguish between myeloid LC and BPDCN.2 CD123 IHC expression has been studied in 157 acute myeloid leukemia (AML) bone marrow biopsies and/or marrow particle preparations, and correlated with the morphologic, immunophenotypic, and cytogenetic features and with the presence of FLT3-ITD and NPM1 mutations.3
CD123 IHC expression has been seen in 40% of AML, across a wide spectrum of 2008 World Health Organization subtypes and was most frequent within the intermediate risk group. Compared with CD123 IHC negative AML, CD123 IHC positive AML demonstrated higher marrow blast percentages (median 69%), monocytic differentiation (33/63 cases), and CD34 negativity (29/63 cases). 83% (25/30) FLT3-ITD-mutated AML were CD123+ and 62% (18/29) NPM1-mutated cases were CD123 IHC+ (P=0.0052). CD123 IHC+AML presents with characteristic pathologic features, some of which may be related to underlying FLT3-ITD and/or NPM1 mutations.3